
Complex PTSD (C-PTSD) affects relationships in ways that are distinct from the effects of standard PTSD. Where PTSD typically develops from a single traumatic event, C-PTSD develops from prolonged, repeated trauma, most often chronic childhood abuse or neglect, long-term domestic violence, or sustained emotional abuse. The relational impact of C-PTSD is not just about avoiding triggers or managing flashbacks. It goes deeper into how the nervous system learned to attach to other people, how it reads threat in intimate relationships, and how it responds when closeness feels dangerous.
If you are in a relationship and C-PTSD is affecting it, or if you love someone with C-PTSD and are trying to understand what you are experiencing together, this article covers the mechanisms, the patterns, and what clinical treatment actually does to change them.
CBH’s South Florida clinical team treats C-PTSD within a comprehensive dual-diagnosis program with verified outcomes. Call 844-503-0126 for a free assessment. All calls are completely confidential.
What Is Complex PTSD and How Is It Different from PTSD?
Post-Traumatic Stress Disorder (PTSD) is a well-recognized condition that develops following exposure to a traumatic event: a single incident of violence, an accident, a natural disaster, or another acutely threatening experience. The core features of PTSD include intrusive re-experiencing of the trauma, avoidance of trauma-related cues, negative alterations in mood and cognition, and hyperarousal.
Complex PTSD, recognized in the ICD-11 and increasingly used clinically in the United States even where it does not yet appear in the DSM-5 as a distinct diagnosis, develops from prolonged and repeated trauma, particularly trauma that occurred in relationships from which escape was difficult or impossible. Childhood abuse and neglect, domestic violence, emotional abuse in long-term relationships, and captivity or coercive control are the most common origins of C-PTSD.
The Three Additional Features of C-PTSD
In addition to the core PTSD features, C-PTSD is characterized by three additional domains that directly affect relationships.
- Emotional dysregulation: difficulty managing intense emotional responses, including emotional flashbacks in which feelings from past traumatic experiences are triggered in the present without necessarily having conscious access to the memory driving them
- Negative self-concept: a deeply held sense of being damaged, defective, worthless, or fundamentally different from other people, often rooted in shame that developed in the context of relational trauma
- Disturbances in relationships: profound difficulty trusting others, oscillating between desperate need for closeness and protective distancing, hypervigilance for signs of rejection or betrayal, and difficulty sustaining stable relationships
These three features, particularly the relational disturbances, are what make C-PTSD so specifically disruptive to intimate relationships and why standard PTSD treatment approaches are often insufficient for people with C-PTSD.
What Causes C-PTSD?
C-PTSD develops from prolonged exposure to traumatic conditions from which escape was psychologically or physically impossible. The most common causes include childhood physical, emotional, or sexual abuse; childhood emotional neglect by caregivers; long-term domestic violence or intimate partner abuse; sustained emotional abuse in adult relationships; human trafficking or other forms of captivity; and chronic exposure to community violence or war. The duration and relational nature of the trauma are what distinguish C-PTSD from standard PTSD. When the source of trauma is a person who was supposed to provide safety, the impact on the capacity for future safe attachment is particularly profound.
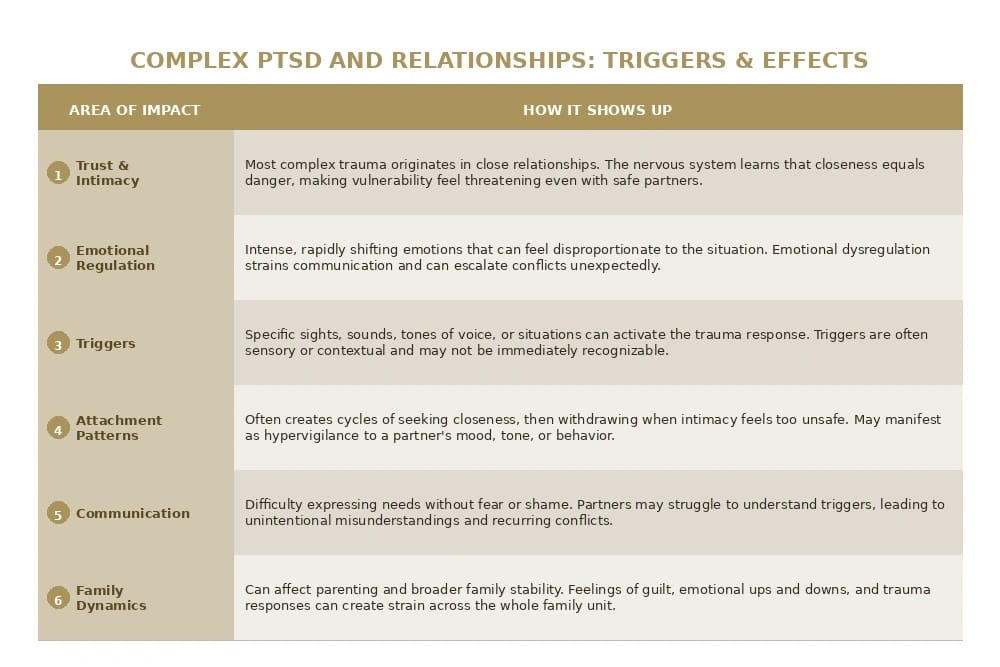
PTSD Effects on Relationships: How C-PTSD Changes Intimacy
C-PTSD affects relationships through several interconnected mechanisms. Understanding these mechanisms, rather than just the surface behaviors they produce, is what allows both the person with C-PTSD and their partner to respond differently.
Hypervigilance for Relational Threat
One of the most consistent effects of C-PTSD on relationships is hypervigilance: a nervous system that is chronically scanning for signs of threat. In the context of relational trauma, this hypervigilance is specifically tuned to interpersonal signals: changes in tone of voice, facial expressions, pauses in communication, changes in a partner’s behavior or mood. These signals are processed by a threat-detection system that was calibrated in an environment where such signals reliably preceded harm.
The result is that a partner’s neutral expression can register as anger. A moment of distance can register as impending abandonment. A minor conflict can activate the same physiological response as a genuinely threatening situation. These responses are not irrational choices. They are the output of a nervous system doing exactly what it learned to do to survive.
Emotional Flashbacks
Emotional flashbacks are one of the most misunderstood features of C-PTSD and one of the most disruptive to relationships. Unlike the visual or sensory flashbacks more commonly associated with PTSD, emotional flashbacks are sudden, intense returns to the emotional states of past traumatic experiences: the terror, shame, helplessness, or worthlessness of childhood abuse, for example, flooding the present without necessarily being accompanied by clear memories.
During an emotional flashback, the person with C-PTSD may not recognize what is happening. They may simply feel suddenly overwhelmed, worthless, terrified, or enraged in a way that seems disproportionate to what is actually occurring in the relationship. Partners often experience this as the person becoming a different person: someone who is no longer accessible, who is responding with an intensity that does not match the situation.
The Push-Pull Pattern
Many people with C-PTSD describe a painful push-pull pattern in intimate relationships: a desperate longing for closeness and connection alongside an equally powerful impulse to create distance when closeness is achieved. Intimacy activates vulnerability. Vulnerability activates the threat response. The nervous system that learned that the people who are supposed to be closest are also the most dangerous responds to intimacy with the same protective withdrawal it developed in the traumatic environment.
Partners experience this as confusing and painful: the person they love seeming to want closeness and then pushing them away, or becoming emotionally unavailable precisely when the relationship feels warmest. Understanding that this is a nervous system response to intimacy itself, rather than a sign of not caring, changes the relational dynamic significantly.
Difficulty Trusting
Trust is the foundational capacity for intimate relationships, and it is precisely what C-PTSD most disrupts. When trust was violated repeatedly by people in positions of authority or attachment, the nervous system learns that trust itself is dangerous. The person with C-PTSD may want to trust their partner and may be aware that their partner has given them no reason not to, while simultaneously being unable to access the felt sense of safety that trust requires.
PTSD and Romantic Relationships: Patterns That Appear Most Often
Abandonment fear in C-PTSD is often deeply rooted in early experiences of emotional neglect or inconsistent caregiving. In adult romantic relationships, this fear can manifest as intense anxiety about a partner’s availability, reassurance-seeking, difficulty tolerating normal periods of distance or independence in the relationship, and disproportionate responses to perceived signs of withdrawal. The fear is real and neurologically grounded even when the actual threat of abandonment is minimal. In romantic relationships specifically, C-PTSD tends to produce several recognizable patterns. These patterns are not unique to every person with C-PTSD but are among the most commonly reported in both clinical practice and by people with lived experience of the condition.
Emotional Numbing and Dissociation
As a protective response to overwhelming emotion, many people with C-PTSD develop the capacity to emotionally disconnect or dissociate. In relationships, this can manifest as sudden emotional unavailability, a flat affect or absence of emotion in situations that call for emotional presence, or a sense of not being fully in the room. Partners often describe this as their loved one seeming to be physically present but emotionally absent, sometimes in the middle of otherwise ordinary interactions.
Difficulty with Conflict
For people whose early relational environment involved conflict that was dangerous or unpredictable, adult relationship conflict can activate the full trauma response even when the actual conflict is normal and non-threatening. The physiological state of conflict, elevated heart rate, tension, raised voices, and emotional intensity, may be indistinguishable to the nervous system from the physiological state of past threatening situations. This can produce either intense conflict escalation or complete shutdown and withdrawal.
Shame and Self-Blame in Relationships
The negative self-concept of C-PTSD, the deep sense of being fundamentally defective or unworthy, affects relationships in specific ways. The person may feel that they do not deserve love or that the relationship’s difficulties are evidence of their essential inadequacy. They may apologize excessively, accept blame for things that are not their responsibility, or sabotage relationships when they feel they are going well because the sense of being loved does not match the internal sense of being unlovable.

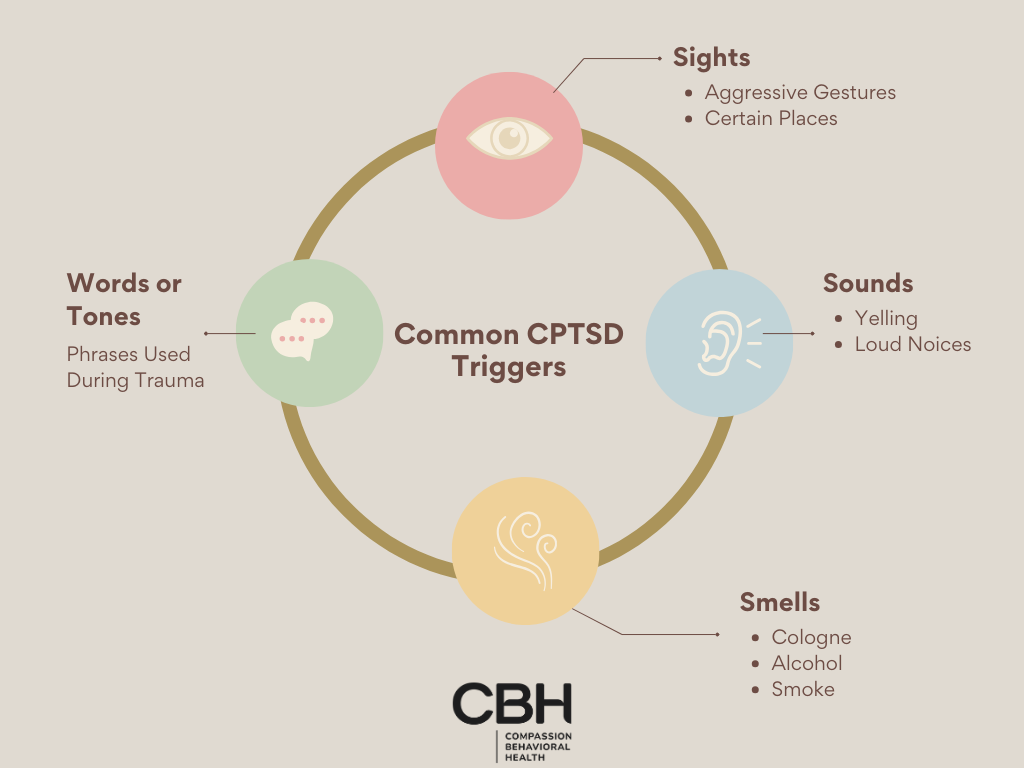
PTSD Triggers in Relationships: What Sets Off the Trauma Response
PTSD triggers in relationships are specific cues, sensory, emotional, situational, or interpersonal, that activate the trauma response in the context of intimate connection. Identifying personal triggers is one of the most important components of C-PTSD treatment because it transforms seemingly random reactivity into understandable patterns.
Common Relationship Triggers for C-PTSD
- Tone of voice: a partner’s raised voice, harsh tone, or even a particular quality of quiet can activate memories of past threatening interactions
- Physical gestures: certain movements, postures, or touches that were associated with past abuse can trigger the threat response even in safe contexts
- Criticism or perceived criticism: any feedback that resonates with the shame narrative of C-PTSD can activate a disproportionate emotional response
- Being ignored or dismissed: particularly activating for people whose trauma involved emotional neglect or having their experiences invalidated
- Conflict or raised voices: activating the physiological state of past threatening situations regardless of actual threat level
- Intimacy and vulnerability: closeness itself can be triggering when the nervous system learned that closeness precedes harm
- Perceived abandonment cues: a partner being late, not responding to messages, seeming distracted, or expressing a need for space
- Specific dates, places, or sensory experiences: anniversaries of traumatic events, locations similar to where trauma occurred, smells or sounds associated with past experiences
PTSD Triggers from Abuse
For people whose C-PTSD developed from domestic violence or emotional abuse, relationship-specific triggers are often particularly intense because the trauma occurred in a relationship context. The very environment of intimate partnership, with its dependency, vulnerability, and emotional intensity, can be triggering in ways that are difficult to explain to a partner who does not understand the history.
Common triggers from abuse include any situation that recreates the power dynamics of the abusive relationship, communication patterns that resemble those of the abuser, feeling controlled or not having choices, and any behavior that resembles tactics used by the abuser even when the current partner’s intent is entirely different.
My Partner Has PTSD and Is Pushing Me Away: What Partners Need to Know
If your girlfriend, boyfriend, spouse, or partner has PTSD or C-PTSD and is pushing you away, pulling back when things feel close, or cycling between intense connection and sudden emotional distance, you are not imagining it and it is almost certainly not about you.
Why People with C-PTSD Push Partners Away
The push-pull pattern in C-PTSD relationships is driven by the nervous system’s learned association between intimacy and danger. As a relationship deepens and the person with C-PTSD becomes more vulnerable, the threat-detection system that was calibrated in a traumatic relational environment becomes more activated, not less. The closeness that is genuinely wanted by one part of the person triggers the protective withdrawal that kept them safe in the past.
This is not a conscious choice, and it is not a reflection of how much the person cares about you. It is the expression of a nervous system doing what it learned to do when the stakes of intimacy felt survival-level. The pushing away is often most intense precisely when the relationship is warmest, because that is when the vulnerability is greatest.
How to Support a Partner with C-PTSD
- Learn about C-PTSD: understanding the mechanisms behind the behaviors transforms confusion and hurt into compassion. The behaviors make sense once you understand the nervous system that produces them
- Do not take the withdrawal personally: the distancing is about a learned threat response, not about your worth or the relationship’s value
- Communicate in low-threat ways: calm, clear, non-blaming communication reduces the likelihood of activating the trauma response
- Respect their pace: pushing for closeness when the person is in a protective withdrawal state often intensifies the withdrawal
- Maintain your own support: caring for a partner with C-PTSD is emotionally demanding. Your own wellbeing matters and your own therapy or support is legitimate
- Encourage professional treatment: C-PTSD responds to treatment. The patterns you are experiencing can change with appropriate clinical support
Taking Care of Yourself
Being in a relationship with someone with C-PTSD can produce its own emotional toll: confusion, loneliness, self-doubt, and secondary stress responses. Your needs in the relationship are valid. Supporting a partner with C-PTSD does not mean having no needs or accepting behaviors that are harmful to you. It means understanding the context of those behaviors while still maintaining appropriate boundaries for your own well-being.
CBH’s Family Program provides support for partners and family members of people in C-PTSD treatment, including psychoeducation about trauma responses and family therapy that addresses the relational system around recovery.
If you are a partner struggling to navigate a relationship affected by C-PTSD, or if you recognize your own trauma patterns in this article and want to understand what treatment could look like for you, CBH’s South Florida team is available. Call 844-503-0126. All calls are completely confidential.

Is Your Relationship Affected by PTSD? Signs to Look For
PTSD and C-PTSD affect relationships in ways that are not always obviously connected to trauma. The following signs may indicate that PTSD is affecting your relationship or that of someone you love.
Signs in the Person with C-PTSD
- Intense emotional reactions that seem disproportionate to what actually happened
- Sudden emotional shutdown or dissociation during conflict or intimacy
- Persistent difficulty trusting a partner despite no evidence of untrustworthiness
- Strong fear of abandonment that affects the relationship regardless of the partner’s actual commitment
- Shame responses that interpret normal relationship friction as evidence of personal defectiveness
- Difficulty accepting love or care without suspicion or deflection
- Cycles of intense closeness followed by protective withdrawal
- Specific triggers that produce strong reactions in the relationship context
Signs in the Relationship Dynamic
- A persistent push-pull pattern that neither partner fully understands
- Communication that regularly escalates or shuts down before resolution
- One partner consistently walking on eggshells to avoid the other’s reactions
- Intimacy that feels uneven or inaccessible even when both partners want connection
- Repeated patterns that both partners recognize but cannot seem to change
- A sense that the relationship is being shaped by something larger than the two people in it

C-PTSD Treatment: What Actually Helps
C-PTSD is treatable. The relational patterns, emotional dysregulation, negative self-concept, and hypervigilance that C-PTSD produces respond to specific, evidence-based clinical approaches. The key is treatment that addresses the trauma directly rather than only managing symptoms.
EMDR for Complex PTSD
Eye Movement Desensitization and Reprocessing (EMDR) is one of the most evidence-supported treatments for PTSD and is endorsed by both the VA and the American Psychological Association as a first-line PTSD treatment. EMDR works by helping the brain reprocess traumatic memories that have been stored in a fragmented, emotionally charged way, allowing them to be integrated into the person’s narrative without the same level of emotional activation.
For C-PTSD, EMDR requires careful pacing and preparation, building stabilization and distress tolerance capacity before processing the traumatic material directly. At CBH, EMDR is available at the PHP and IOP levels for clients with C-PTSD, with the clinical team monitoring mood stability and readiness throughout. CBH’s verified 88% improvement in PTSD outcomes reflects a program that treats trauma directly with appropriate clinical rigor.
DBT for Emotional Dysregulation
Dialectical Behavior Therapy provides the specific skill set that addresses the emotional dysregulation component of C-PTSD: mindfulness for observing emotional states without being overwhelmed by them, distress tolerance for surviving emotional flashbacks and crisis states without destructive behavior, emotional regulation for understanding and modulating intense emotional responses, and interpersonal effectiveness for navigating the relational challenges that C-PTSD produces.
Trauma-Focused CBT
Cognitive Behavioral Therapy approaches adapted for trauma address the negative cognitions that C-PTSD produces: the beliefs about being fundamentally defective, unlovable, or responsible for the trauma that occurred. Restructuring these beliefs directly reduces the shame and negative self-concept that so significantly affect intimate relationships.
C-PTSD Treatment at CBH in South Florida
CBH treats Complex PTSD and PTSD within a comprehensive dual-diagnosis residential and outpatient program at its South Florida facilities. Medical detox and residential treatment are in Hollywood, FL. PHP and IOP, where EMDR and DBT are delivered in the context of community reintegration, are in Fort Lauderdale, FL. The same clinical team and the same psychiatrist serve clients from the first day of residential through the last day of IOP, with no handoff gaps in the therapeutic relationship.
- EMDR at the PHP and IOP levels for trauma processing
- DBT across all levels of care for emotional regulation and interpersonal skills
- Family therapy beginning at PHP, addressing the relational system around C-PTSD recovery
- 88% improvement in PTSD outcomes, verified by Greenspace Health across more than 1,000 patient surveys
- Dr. Daud, board-certified in psychiatry and addiction psychiatry, overseeing all evaluations
- In-network with Aetna, Blue Cross Blue Shield, Cigna, Optum, TRICARE East, and the VA
- PsychArmor certified for military-competent care
Complex PTSD and Relationships Q&A
How does complex PTSD affect relationships?
Complex PTSD affects relationships primarily through four interconnected challenges: hypervigilance (a constant state of scanning for threat that can read as distrust or paranoia to a partner), emotional dysregulation (intense and rapidly shifting emotional responses that are disproportionate to the immediate situation), difficulty with trust and intimacy (rooted in the interpersonal nature of most complex trauma), and a tendency toward either anxious attachment or avoidant withdrawal. These patterns are trauma responses, not character flaws, and respond well to targeted treatment such as EMDR and trauma-focused therapy.
What are CPTSD triggers in relationships?
Common CPTSD triggers in relationships include perceived abandonment or rejection (even minor, such as a partner being briefly unresponsive), raised voices or a particular tone of voice, physical touch in certain contexts, feeling controlled or criticised, perceived dishonesty, sudden changes in a partner’s mood or behaviour, and situations that resemble the original traumatic environment. Triggers are often not obvious; they can be sensory, emotional, or contextual, and may not be immediately recognisable to the person experiencing them.
What are common CPTSD triggers specifically?
The most commonly reported CPTSD triggers include: raised voices or aggressive tone, being ignored or dismissed, physical proximity or touch in certain situations, conflict or confrontation, perceived criticism or rejection, witnessing others in distress, feeling trapped or controlled, anniversaries or sensory reminders of traumatic events, and sleep deprivation or extreme stress (which lowers the threshold for triggering). Triggers operate through the nervous system rather than through conscious thought, which is why people with CPTSD often feel confused or ashamed by their intensity.
How do you support someone with CPTSD?
The most effective ways to support someone with CPTSD are to learn about the condition (understanding that their responses are neurological, not personal), to be consistent and predictable (unpredictability is a major trigger), to avoid taking triggered reactions personally, to ask what kind of support they need rather than assuming, to maintain your own boundaries compassionately, and to encourage professional treatment. Supporting someone with CPTSD is not the same as treating it; the most helpful thing a partner or loved one can do is be a regulated, safe presence while the person accesses appropriate therapeutic support.
How do you help someone with CPTSD?
Helping someone with CPTSD involves both practical and emotional support. Practically: helping them access trauma-informed therapy (EMDR, somatic therapy, or trauma-focused CBT are particularly effective), supporting routine and stability, and reducing environmental stressors where possible. Emotionally: validating their experience without minimising it, learning their specific triggers so you can avoid unnecessary activation, being patient with slow progress, and not attempting to be their therapist. It is equally important that the supporting person accesses their own support; secondary traumatic stress is real and common in people closely supporting someone with CPTSD.
What is the worst thing you can do to someone with Complex PTSD?
The worst things you can do to someone with complex PTSD are: dismissing or minimising their trauma (“that was a long time ago” or “other people have it worse”), being unpredictable or inconsistent in your behaviour, pressuring them to “get over it” or move faster than their nervous system can manage, attempting to force physical contact or emotional closeness they haven’t initiated, threatening abandonment during conflict, and exposing them to their known triggers without warning or consent. These actions reinforce the core wounds of CPTSD: that the world is unsafe, that their feelings are invalid, and that people cannot be trusted.
What does CPTSD look like in romantic relationships?
In romantic relationships, CPTSD often presents as intense early attachment followed by anxiety about the relationship’s security, difficulty communicating needs without feeling shame or fear, hypervigilance to a partner’s mood and behaviour, strong reactions to perceived rejection or abandonment, periods of emotional withdrawal or shutdown, difficulty with sexual or physical intimacy, and recurring relationship conflicts that feel circular and unresolvable. Both partners are affected — the person with CPTSD by their trauma responses, and their partner by the unpredictability and emotional intensity that can accompany them.
Can you get PTSD from a relationship?
Yes, repeated emotional, psychological, or physical abuse within a relationship is a recognised cause of complex PTSD. Unlike single-incident PTSD, relational PTSD develops from sustained exposure to threat, control, humiliation, or unpredictability, particularly in intimate relationships where escape feels impossible. Symptoms include hypervigilance, emotional numbing, intrusive memories, difficulty trusting future partners, and a distorted sense of self. PTSD from a relationship is clinically recognised and responds to the same evidence-based treatments as other forms of complex PTSD.
Can PTSD from an abusive relationship be treated?
Yes, PTSD from an abusive relationship is very treatable, particularly with trauma-focused therapies. EMDR (eye movement desensitisation and reprocessing) has strong clinical evidence for reducing the intensity of traumatic memories and associated symptoms. Trauma-focused CBT, somatic therapies, and schema therapy are also effective. Recovery typically involves processing the traumatic experiences, rebuilding a stable sense of self, and developing new relational patterns. Many people with relational PTSD achieve significant symptom reduction and go on to have healthy, secure relationships.
How does CPTSD affect trust in relationships?
CPTSD fundamentally disrupts the capacity for trust because most complex trauma originates in relationships, particularly with caregivers or intimate partners, where trust was repeatedly violated. The nervous system learns that closeness equals danger, creating a paradox: the person deeply needs connection but experiences intimacy as threatening. This can manifest as constant testing of a partner’s loyalty, interpreting neutral behaviour as threatening, difficulty believing positive intentions, or cycles of seeking closeness and then withdrawing when it feels too vulnerable.
What are PTSD triggers from abuse specifically?
PTSD triggers from abuse are stimuli that activate the trauma response because they share sensory, emotional, or contextual features with the original abuse. Common triggers from abusive relationships include specific tones of voice or facial expressions used by the abuser, being in enclosed spaces, certain phrases or words, physical touch in particular ways, a partner raising their voice, smells or sounds associated with the abusive environment, and situations involving perceived control or powerlessness. The nervous system doesn’t distinguish between past and present threats; the trigger produces the same physiological response as the original event.
What is CPTSD, and how is it different from PTSD?
Complex PTSD (CPTSD) and PTSD share core symptoms, intrusive memories, hypervigilance, and avoidance, but CPTSD additionally includes three symptom clusters specific to complex, repeated trauma: affect dysregulation (difficulty managing emotional responses), negative self-concept (deep shame, worthlessness, or a sense of being permanently damaged), and disturbances in relationships (difficulty trusting others, feeling detached, or patterns of revictimisation). PTSD typically follows a single traumatic event, while CPTSD develops from prolonged, repeated exposure, most commonly childhood abuse, domestic violence, or captivity.
How does CPTSD affect intimacy and sexuality?
CPTSD frequently affects sexual and physical intimacy because trauma is stored in the body as well as the mind. People with CPTSD may experience dissociation during physical contact, strong aversion to certain types of touch, difficulty being present during sex, shame or disgust responses that feel disconnected from the immediate situation, or hypersexuality as a coping mechanism. These responses are trauma symptoms, not reflections of desire or attraction to a partner. Somatic therapy and trauma-informed sex therapy can be particularly effective for addressing intimacy-related CPTSD symptoms.
Does complex PTSD cause relationship sabotage?
Yes. Relationship sabotage is a recognised pattern in CPTSD, often driven by the unconscious expectation that closeness will result in pain. When a relationship feels “too good” or when a person with CPTSD begins to feel genuinely safe, the nervous system can interpret this unfamiliar safety as a threat, triggering behaviours that push the partner away, conflict escalation, emotional withdrawal, or testing behaviours. This is not intentional self-sabotage but a survival response learned in environments where closeness reliably preceded harm. Therapy that directly addresses this pattern can interrupt the cycle.
How does CPTSD affect anger and conflict in relationships?
Short answer: CPTSD is associated with significant difficulties in anger regulation, not because people with CPTSD are aggressive by nature, but because their nervous system is chronically dysregulated and their threshold for perceived threat is much lower than in people without trauma histories. Conflict can trigger a full fight-or-flight response, producing anger that feels disproportionate to the situation. Conversely, some people with CPTSD suppress anger entirely (having learned it was unsafe to express) and implode rather than explode. Both patterns create relational difficulties, and both respond to emotion regulation work in therapy.
Can complex PTSD cause jealousy in relationships?
Yes, jealousy is common in CPTSD relationships and is typically driven by hypervigilance (scanning for signs of abandonment or betrayal), a deep-seated belief that the person is unworthy of love and will inevitably be left, and a history in which infidelity or abandonment was a feature of past trauma. The jealousy is usually not about the partner’s actual behaviour but about the trauma history being activated. While the experience of jealousy feels very real, it often causes significant relational harm and is one of the patterns most important to address in trauma therapy.
What does a CPTSD episode look like?
A CPTSD episode is an acute activation of the trauma response, typically triggered by something in the current environment that the nervous system associates with past danger. It can involve intense emotional flooding (overwhelming fear, rage, shame, or grief), physical symptoms (shaking, dissociation, inability to speak, heart racing), complete emotional shutdown or freezing, a sudden collapse into past trauma memories or sensory experiences, or explosive emotional reactions. Episodes typically last from minutes to hours and are often followed by exhaustion, shame, and confusion about what triggered the response.
How does CPTSD affect marriage and long-term relationships?
In long-term relationships and marriages, CPTSD creates recurring challenges around emotional safety, conflict management, and intimacy. Partners often describe feeling like they are “walking on eggshells,” unsure of what will trigger a response. The person with CPTSD may struggle with commitment anxiety, emotional availability, and the vulnerability that long-term closeness requires. Marriages where one partner has CPTSD benefit significantly from couples therapy alongside individual trauma treatment, particularly approaches that help both partners understand the trauma responses and develop co-regulation skills together.
How do CPTSD and divorce relate?
Complex PTSD and divorce intersect in two ways. First, CPTSD can be caused by a marriage characterised by abuse, control, or chronic emotional neglect, with divorce being the aftermath of relational trauma. Second, divorce itself can be deeply triggering for someone with pre-existing CPTSD, activating abandonment fears, identity dissolution, and profound instability. In both cases, trauma-informed therapeutic support during and after divorce is strongly recommended. Court proceedings involving custody disputes are particularly activating for people with CPTSD and often benefit from advocacy support alongside therapy.
How do you explain CPTSD to a partner?
Explaining CPTSD to a partner is most effective when framed around the nervous system rather than personal history, describing it as a survival system that learned to stay on high alert rather than a character trait or choice. Useful frameworks include explaining triggers as automatic alarms rather than deliberate reactions, describing the difference between feeling emotionally flooded and wanting to hurt someone, being honest about specific known triggers so the partner can understand what to avoid, and sharing what co-regulation helps (such as a calm presence, space, or physical grounding). Many people find doing this with a therapist present helpful.
Can someone with CPTSD have a healthy relationship?
Yes. Many people with CPTSD maintain loving, stable, and healthy relationships, particularly with appropriate therapeutic support. CPTSD is a treatable condition, and with effective treatment, the intensity and frequency of trauma responses can be reduced significantly. The key factors for relationship health are the person with CPTSD being in active treatment, both partners having realistic expectations about the process of recovery, the non-CPTSD partner having their own support system, and both people developing trauma-informed communication and co-regulation skills. Recovery is not linear, but healthy relationships are absolutely achievable.
What is the impact of CPTSD on family relationships and parenting?
CPTSD can affect parenting and family relationships through emotional dysregulation (which can be frightening for children even without abuse occurring), hypervigilance that creates an atmosphere of tension, difficulty with the vulnerability and dependency that parenting requires, and a tendency to be triggered by a child’s distress or neediness if these resemble the person’s own childhood experiences. Many parents with CPTSD are deeply devoted and motivated to parent differently than they were parented. Trauma-informed parenting support and individual therapy can significantly improve outcomes for both parent and child.
What is PTSD from domestic violence, and how is it treated?
PTSD from domestic violence is a form of complex PTSD that develops from repeated exposure to physical, emotional, psychological, or sexual abuse within an intimate relationship. Symptoms include hypervigilance, startle responses, intrusive memories of abusive incidents, avoidance of reminders, emotional numbing, difficulty trusting new relationships, and profound disruption to self-worth. Treatment is most effective when it combines safety planning, trauma-focused therapy (particularly EMDR and trauma-focused CBT), and, where appropriate, group-based support with other survivors. The therapeutic relationship itself is often healing, as it provides a corrective experience of a safe interpersonal connection.
How does PTSD affect romantic relationships?
PTSD and Complex PTSD affect romantic relationships through several mechanisms: hypervigilance for interpersonal threat that causes neutral partner behavior to register as danger; emotional flashbacks that flood the present with past traumatic emotional states; a push-pull pattern of intense closeness followed by protective withdrawal driven by the nervous system’s association between intimacy and danger; difficulty trusting even a partner who has given no reason for distrust; and emotional numbing or dissociation that creates distance during moments that call for emotional presence.
What are PTSD triggers in relationships?
Common PTSD triggers in relationships include a partner’s tone of voice or facial expression that resembles past threatening interactions; criticism or perceived criticism that activates shame; conflict or raised voices; perceived abandonment cues such as a partner being unavailable or seeming distant; intimacy and vulnerability themselves; and specific sensory experiences associated with past trauma. For people with C-PTSD from domestic or emotional abuse, triggers often recreate the dynamics or patterns of the abusive relationship even when the current partner’s intent is entirely different.
Can emotional abuse cause PTSD?
Yes. Emotional abuse can cause both PTSD and Complex PTSD. Sustained emotional abuse, including criticism, humiliation, gaslighting, coercive control, and isolation, produces the same neurological changes as physical trauma. The chronic stress response activated by prolonged emotional abuse alters the brain areas involved in threat detection and emotional regulation, producing hypervigilance, intrusive re-experiencing, avoidance, and emotional dysregulation. C-PTSD is particularly common in survivors of long-term emotional abuse because the prolonged and relational nature of this trauma matches the conditions under which C-PTSD develops.
Why does my partner with PTSD push me away?
A partner with PTSD or C-PTSD pushing you away is typically an expression of the nervous system’s learned association between intimacy and danger. As the relationship deepens and vulnerability increases, the threat-detection system calibrated in a traumatic relational environment activates protective withdrawal. This is most intense when the relationship is closest because that is when vulnerability is greatest. It is not a reflection of how much your partner cares about you. It is a trauma response that can change with appropriate clinical treatment.
Is your relationship affected by PTSD?
Signs that PTSD may be affecting your relationship include: disproportionate emotional reactions to routine relationship friction; cycles of intense closeness followed by sudden emotional withdrawal; persistent difficulty trusting despite no evidence of untrustworthiness; strong abandonment fear that affects the relationship regardless of your commitment; communication that regularly escalates or shuts down before resolution; and a sense that both partners are stuck in patterns neither can change. These patterns are clinical signals, not personal failures, and they respond to treatment.
What is the difference between PTSD and Complex PTSD?
PTSD typically develops from a single traumatic event and is characterized by intrusive re-experiencing, avoidance, negative mood changes, and hyperarousal. Complex PTSD develops from prolonged, repeated trauma, especially relational trauma in which escape was difficult, and includes all PTSD features plus three additional domains: emotional dysregulation, negative self-concept rooted in shame, and profound disturbances in relationships including difficulty trusting others and oscillating between desperate need for closeness and protective distancing.
Does CBH treat Complex PTSD in South Florida?
Yes. CBH treats Complex PTSD and PTSD at its South Florida residential program in Hollywood and outpatient PHP and IOP programs in Fort Lauderdale. EMDR is available for trauma processing at the PHP and IOP levels. DBT is delivered across all levels of care. Family therapy addresses the relational system around C-PTSD recovery. CBH’s verified outcomes include 88% improvement in PTSD symptoms across more than 1,000 patient surveys by Greenspace Health. Call 844-503-0126 for a free clinical assessment.

C-PTSD in Relationships Can Change
The relational patterns that C-PTSD produces- the push-pull, the hypervigilance, the emotional flashbacks, the difficulty trusting- are not permanent features of the person who has them. They are the learned responses of a nervous system that did what it had to do to survive. With the right clinical treatment, those responses can change. The capacity for intimacy that C-PTSD obscures does not disappear. It waits.
If you or someone you love is living with the effects of complex trauma in your relationships, CBH’s South Florida team is here. Whether you are the person with C-PTSD trying to understand yourself, or the partner trying to understand what is happening between you, there is a path forward that does not require either of you to stay in the same place.
Call 844-503-0126. Available 24 hours a day, seven days a week. All calls are completely confidential. Insurance verified at no cost. Stories change here.
Ryan attended college at the Ohio State University and the University at Buffalo, receiving degrees in Sociology. His background and experience in the healthcare space has led him to his role as a managing partner at Compassion Behavioral Health. Ryan demonstrates a strong ability to identify project needs, formulate strategies, maintain good practice quality assurance, and manage a team to deliver the highest standard of client care and professionalism.


